Chest Radiology > Pathology > Pulmonary Embolus
Pulmonary
Embolism
![]()
Pulmonary embolism (PE) is not uncommon in the inpatient setting. The primary
source is thrombus from the deep veins of the legs. Roughly ten percent of
pulmonary embolisms result in pulmonary infarction, but many patients die of PE
without being diagnosed. The primary purpose of a chest film in
suspected PE is to rule out other diagnoses as a cause of dyspnea or hypoxia.
Most CXRs in patients with a PE are normal. Signs that may be present in PE are; Westermark's sign (oligemia in area of involvement), increased size of a hilum
(caused by thrombus impaction), atelectasis with elevation of hemidiaphragm and
linear or disk shaped densities, pleural effusion, consolidation, and Hampton's
hump (rounded opacity). In the case of pulmonary infarctions, the main
radiographic feature is multifocal consolidation at the pleural base in
the lower lungs. Several other important modalities are used when
investigating possible PE. These modalities are venous ultrasound, V/Q scan,
pulmonary arteriogram, and CT angiogram (CTA). Remember, if the CXR of a
patient with hypoxia is normal you should consider PE.
The workup of suspected PE can be divided into two populations. In the inpatient setting a CTPA will likely be more definitive than a V/Q scan, as it may disclose other causes of hypoxia not shown on CXR. If the patient has leg swelling, a venous ultrasound of the leg veins should be done to exclude DVT. In the outpatient setting a V/Q scan should be the first test and will less likely be indeterminate than in the inpatient setting. There is also a lower radiation dose for V/Q scans than for CTPA. If these studies are inconclusive a pulmonary arteriogram is the definitive, but more invasive test.
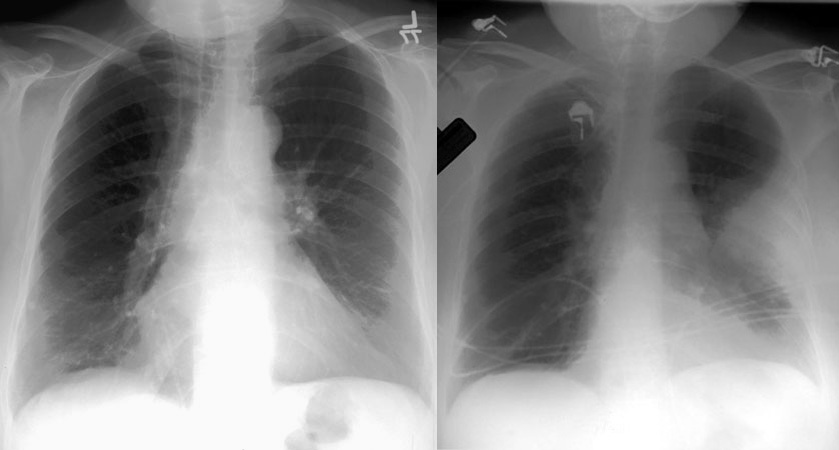
These are two PA exams demonstrating
Hampton's hump (rounded perioheral
opacities) in patients with pulmonary embolism.
What is the most common chest x-ray finding in PE? (Click for answer)
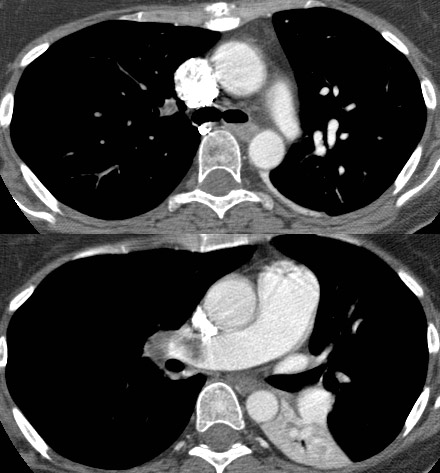
Above are 2 CT scans from the
same patient demonstrating a large pulmonary embolus.
Which vessel is it affecting? (Click for answer and arrows)
![]()
![]()
© Copyright Rector and Visitors of the University of Virginia 2013