Gastrointestinal Radiology > Post-Test Answers
Post-Test Answers
![]()
|
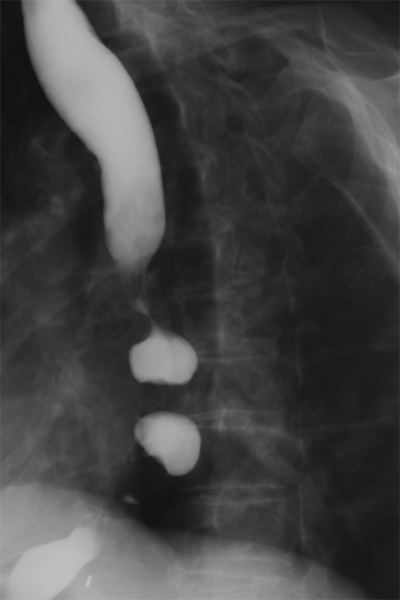
1. The appearance of the esophagus below is typical of what disease process:
A. Chagas' disease B. Scleroderma C. Diffuse esophageal spasms D. Achalasia C: This esophagram shows the typical "corkscrew" or "beaded" appearance of diffuse esophageal spasms. |
||
|
2. The classic radiographic features of Barrett's esophagitis are high esophageal strictures or deep penetrating ulcers. True False TRUE: The classic radiologic features of Barrett's consist of high esophageal strictures or deep, penetrating ulcers that are also associated with a sliding hiatal hernia and gastroesophageal reflux. The "high" location of these strictures and ulcers is attributed to fact that they occur at the squamocolumnar junction in the midesophagus. |
||
|
3. The majority of esophageal carcinomas are of the adenocarcinoma type. True False FALSE: In the esophagus, a majority of carcinomas are of the squamous cell type. |
||
|
4. Which of the following is NOT included in the differential diagnosis of enlarged gastric folds? A. Zollinger-Ellison Syndrome B. Linitis Plasitca C. Lymphoma D. Corrosive Gastritis E. Menetrier's Disease B.: Linitis plastica is associated with infiltrating gastric malignancies which result in diffuse wall thickening and loss of rugae. All of the other conditions listed are associated with enlarged gastric folds and are therefore not correct answers. |
||
|
5. All of the following statements regarding gastric imaging are true EXCEPT: A. Water soluble contrast should be used if a leak or perforation are suspected. B. A double contrast upper GI series uses both oral and IV contrast. C. A double contrast study provides improved mucosal visualization. D. The imaging study of choice for diagnosing hypertrophic pyloric stenosis is ultrasonography. B.: A double contrast study utilizes ingested oral contrast and air (not IV contrast) to coat the mucosa and distend the stomach, providing enhanced mucosal detail. |
||
|
6. The image below is from a single contrast barium study in a 46 year old male following gastrojejunostomy. Based upon the findings below, what is the diagnosis?
A. Afferent limb syndrome B. Bile reflux gastritis C. Normal postoperative Bilroth II D. Gastric stump cancer E. Anastomotic leak A: The UGI image demonstrates Afferent Limb Syndrome. The afferent limb is non-opacified (obstructed) and is dilated due to the accumulation of GI secretions. The efferent limb is patent. |
||
|
7. What is the most common sequela of a Meckel's diverticulum? A. Asymptomatic B. GI bleeding C. Obstruction D. Perforation E. Cancer A: Meckel's diverticulum is a relatively common congenital abnormality, reportedly present in up to 2% of the general population. This remnant of the vitelline duct invariably resides on the antimesenteric side of the distal ileum within two feet of the ileocecal valve. It most commonly presents as an incidental finding on imaging studies performed for other reasons. Symptomatic children usually present with obstruction, while symptomatic adults usually present with GI bleeding. |
||
|
8. What structure is being imaged here?
A. Stomach B. Ligament of Treitz C. Terminal ileum D. Rectum C: This is a magnified spot film of the terminal ileum during a single-contrast small bowel follow-through. Careful evaluation of the terminal ileum is necessary for a complete SBFT because of its propensity to be involved in small bowel disease. Several inflammatory, infectious, and neoplastic processes can cause isolated disease. Evaluation of the terminal ileum may be enhanced with prone compression views or peroral pneumocolon. Prone compression views entail using a paddle to compress the right lower quadrant while the patient lies on their stomach. Peroral pneumocolon entails infusion of air through a rectal tube until air is refluxed through the colon and ileocecal valve into the terminal ileum. This allows for a doulbe-contrast evaluation of the terminal ileum and a more sensitive view of the mucosal surface. |
||
|
9. What is the salient finding in the image in the above question? A. Stricture B. Fistula C. Bowel dilatation D. A and B E. All of the above D: There is marked, smooth narrowing of the terminal ileum as it arcs rightward into the ileocecal junction. This is the typical appearance of a stricture. In addition, there are at least two linear tracts emanating leftward, which represent fistulas. Fistulas may aberrantly connect the small bowel to the vagina (enterovaginal), skin (enterocutaneous), bladder (enterovesicular), small bowel (enteroenteral), or colon (enterocolic). |
||
|
10. What is the abnormality in the image below?
A. Filling defect B. Luminal dilatation C. Stricture D. Fistula A: Spot film of the terminal ileum demonstrates a round filling defect. |
||
|
11. From where is the mass in the above image likely arising? A. Bowel lumen B. Bowel mucosa C. Bowel wall D. Extrinsically B: The morphology of a filling defect can help to decipher its location. This mass demonstrates acute angles where it meets the bowel wall, suggesting a mucosal or submucosal location. Intramural (leiomyoma) and extrinsic masses demonstrate margins with more obtuse angles with the bowel wall. |
||
|
12. The following image demonstrates a complication seen most often due to: A. Appendicitis with a ruptured appendix B. Metastatic carcinoid tumor C. Metastatic mucinous adenocarcinoma C: The image is an example of pseudomyxoma peritonei, most often secondary to metastatic mucinous adenocarcinoma. The key in this image is to recognize that the mass effect exerted on the small intestines by the gelatinous matrix of pseudomyxoma peritonei.
|
||
|
13. What are the dimensions of the normal appendix as seen on ultrasound: A. 7 cm x 2 cm B. 7 mm x 2 mm C. 7 in x 2 in D. None of the above D: The normal appendix cannot be visualized on ultrasound |
||
|
14. Ischemic colitis is usually caused by an arterial occlusion.
|
||
|
15. Which of the following is malrotation NOT associated with?
|
||
|
16. Intussusception may be caused by any of the following EXCEPT:
|
||
|
17. Which of the following can be used to differentiate a paralytic ileus from a partial small bowel obstruction?
|
||
|
18. Patients with suspected toxic megacolon should have a barium study to confirm diagnosis.
|
||
|
19. Sigmoid volvulus is more common than cecal volvulus.
|
||
|
20. During what contrast phase is a hepatocellular carcinoma most likely to enhance? A. Arterial phase B. Portal venous phase C. Equilibrium phase A: Primary malignancies of the liver typically have hepatic arterial supply, thus will enhance during the arterial phase. Normal liver parenchyma has primarily portal venous supply, therefore, enhances during portal venous phase of I.V. contrast. |
||
|
21. All of the following are signs of advanced cirrhosis on imaging EXCEPT: A. Liver surface nodularity B. Contracted liver with ascites C. Atrophy of the posterior segments (VI,VII) of the right lobe D. Enlarged caudate lobe (I) and lateral segments (II,III) of the left lobe E. Prominent umbilical vein F. Irregular enhancement G. All of the above are signs of advanced cirrhosis G: All of the above are signs of advanced cirrhosis on imaging |
||
|
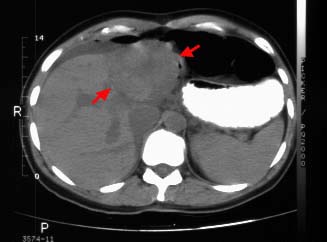
22. The following image depicts hepatic hemangioma.
True False FALSE: The image shows focal nodular hyperplasia. Noncontrast CT shows the lesion has low attenuation (arrows) compared with normal liver. The central stellate scar also shows low attenuation. |
||
|
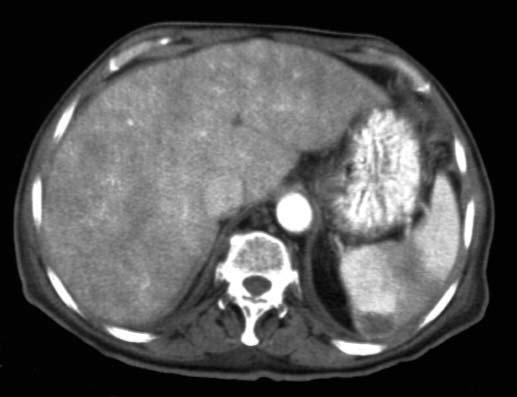
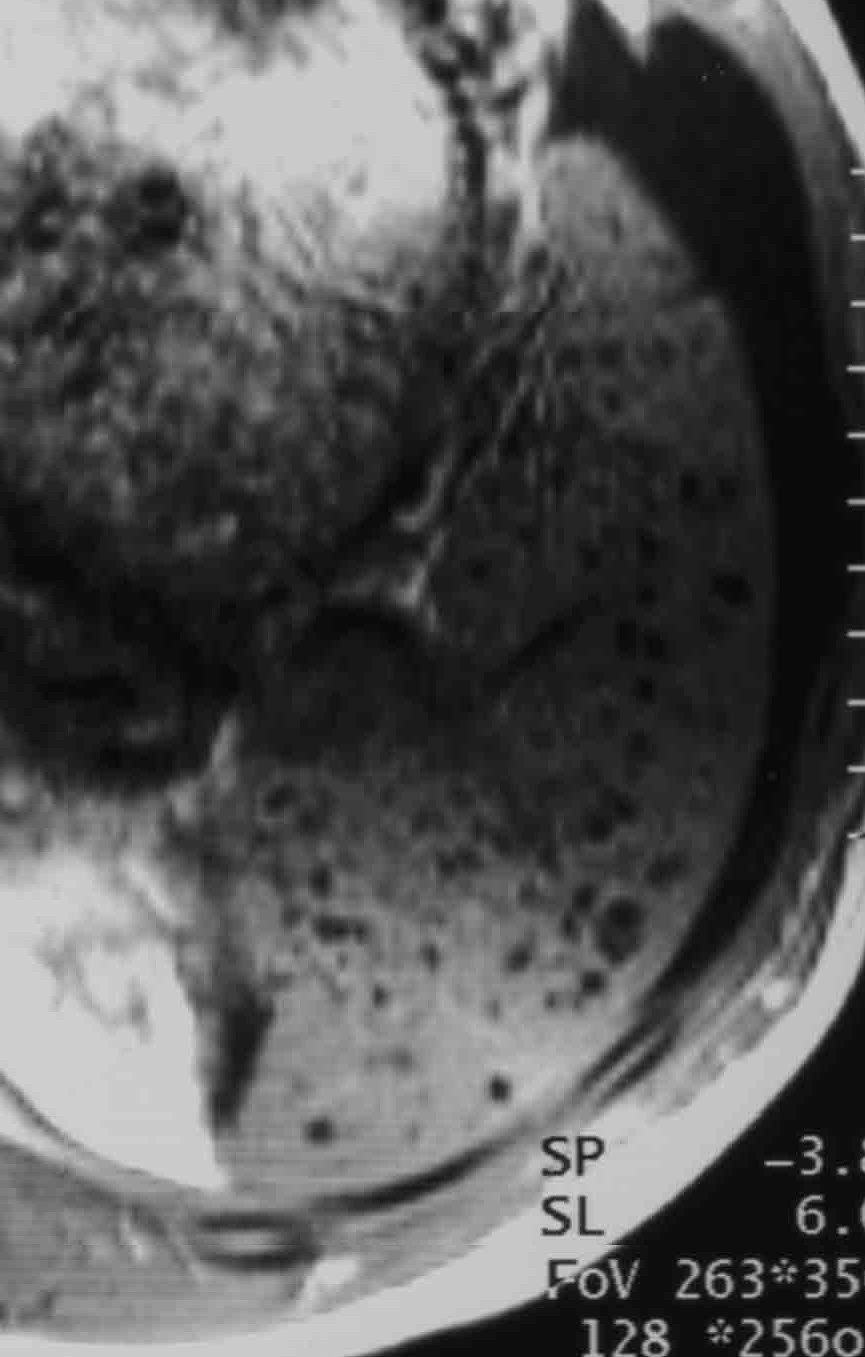
23. The appearance of the liver below is due to:
A. CHF B. Constrictive pericarditis C. Restrictive cardiomyopathy D. Any of the above D: The image depicts passive hepatic congestion, also known as nutmeg liver due to its appearance. The liver is enlarged without focal disease. The areas of low attenuation are caused by chronic increased hepatic venous pressure. |
||
|
24. The upper limit of normal for the dimensions of a normal gallbladder are: A. 10 cm long, 3 cm wide B. 15 cm long, 5 cm wide C. 5 cm long, 3 cm wide D. 20 cm long, 5 cm wide E. 15 cm long, 10 cm wide A: The dimensions of a normal, non-dilated gallbladder are 10 cm long x 5 cm wide. Dimensions larger than these parameters are considered dilated, and could indicate underlying pathology or obstruction. |
||
|
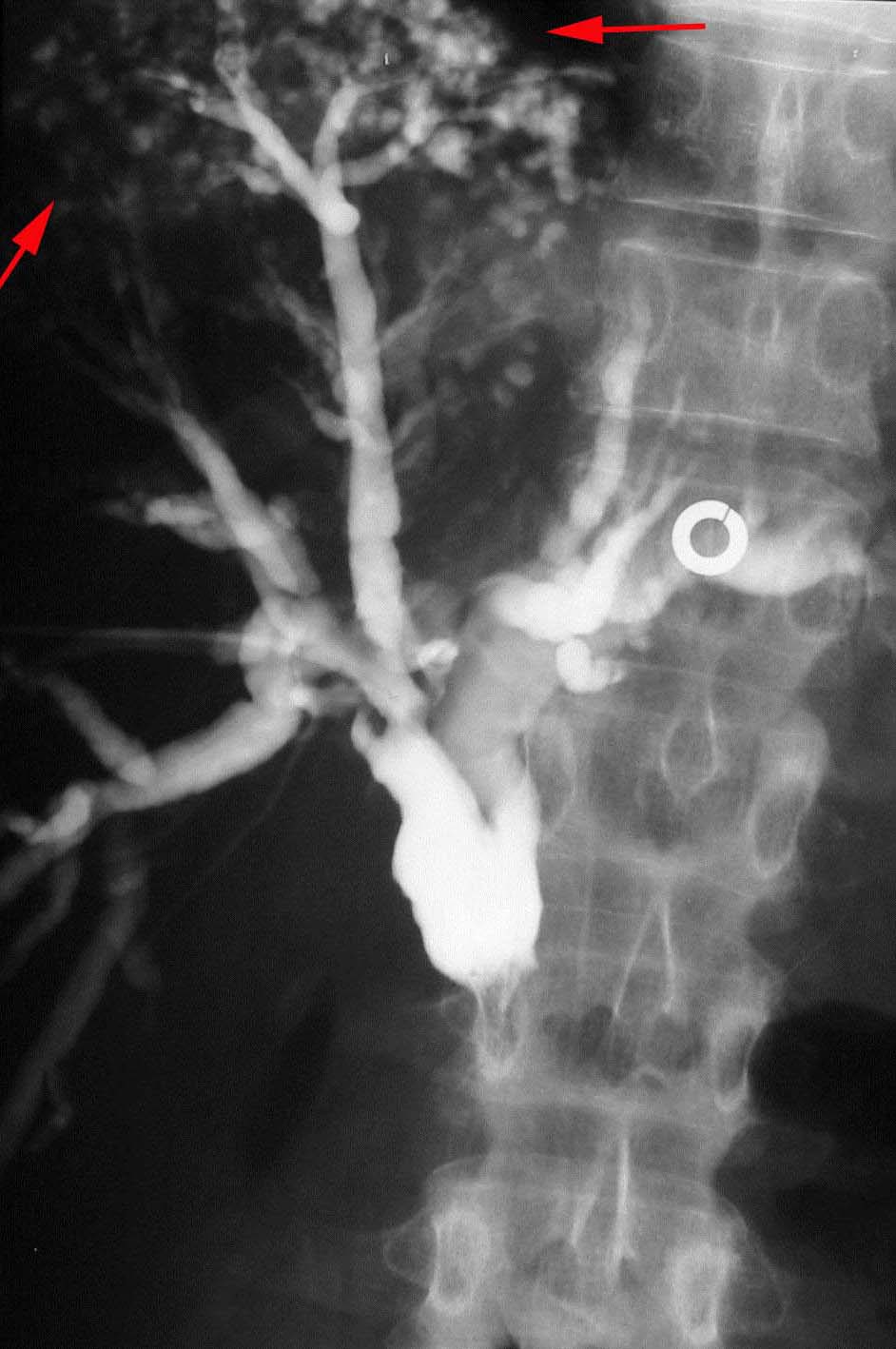
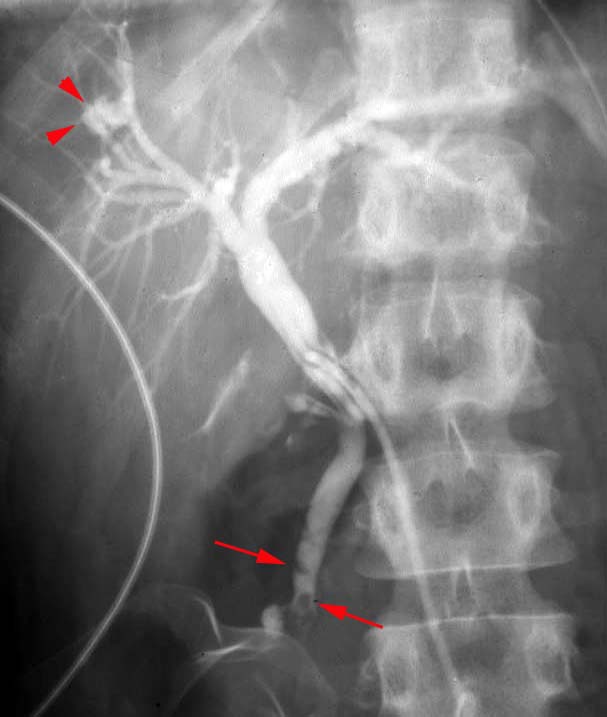
25. What condition does the following image most likely represent? A. Ascending cholangitis B. Biliary obstruction C. Mirizzi's syndrome
A: The pathogenesis of ascending cholangitis is gram negative bacterial infection. Patients present with abdominal pain, fever, and obstructive LFTs. Associated radiographic findings early during the process reveal nothing but an obstructive pattern. Later findings reveal pleating or wall irregularity, mural necrosis and even intrahepatic abscesses at duct ends (as demonstrated by red arrows on the right image above). |
||
|
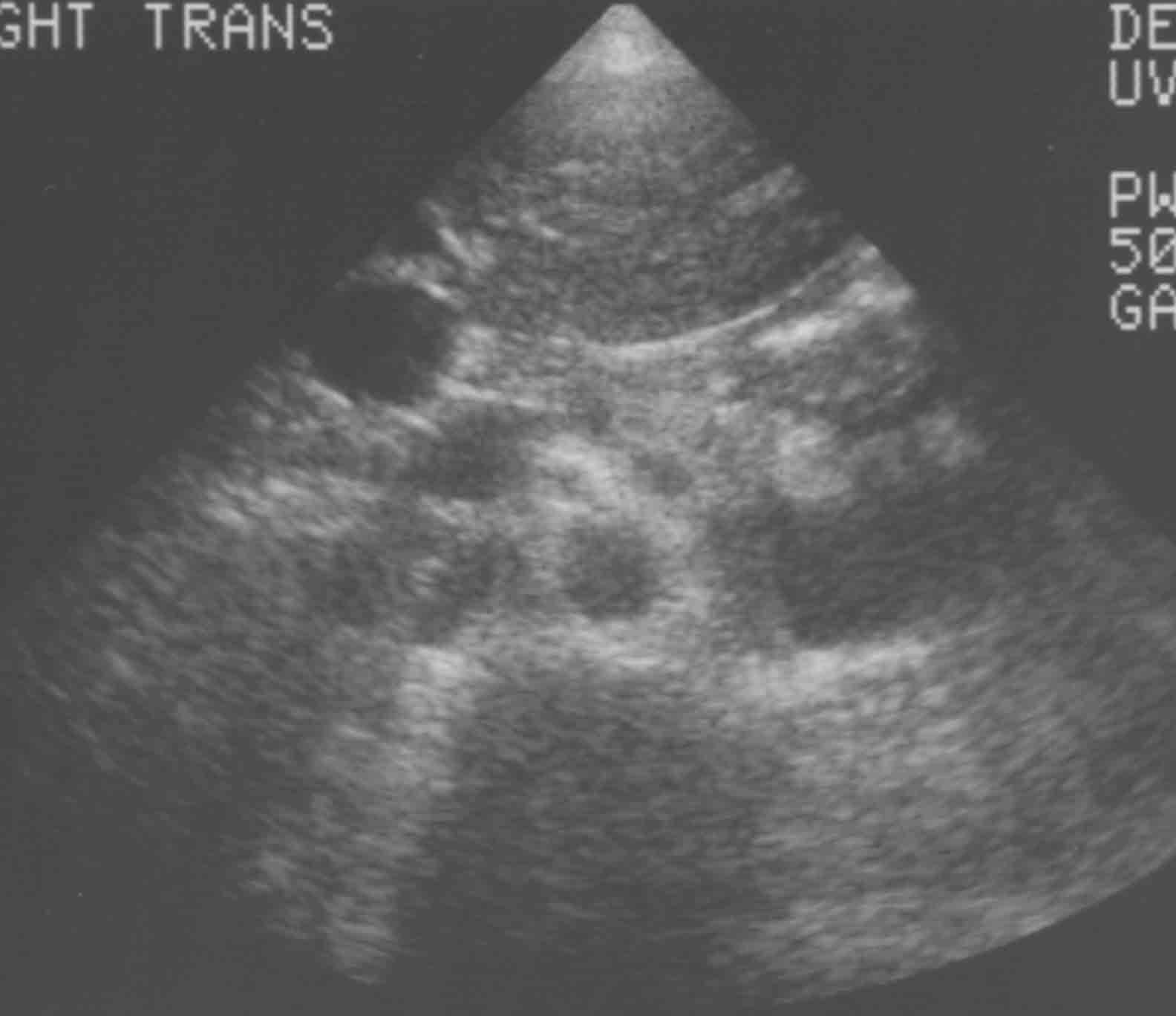
26. Caroli’s Disease is a type of choledochal cyst characterized by: A. Solitary fusiform extrahepatic cyst B. Extrahepatic supraduodenal diverticulum C. Intraduodenal diverticulum choledochocele D. Multiple intrahepatic cysts
D: A rare disorder characterized by saccular intrahepatic duct dilations with stones and strictures. Usually presents in adults as right upper quadrant pain, fever, and jaundice. Predisposes one to stones, cholangitis, liver abscess, hepatic fibrosis, portal hypertension. Treatment involves antibiotics, biliary drainage, and stone removal. However, overall prognosis is poor. |
||
|
27. All the following are radiographic signs of annular pancreas except: A. Double bubble sign B. Prenatal hydroamnios C. Minimal distal bowel gas D. Crescent sign D: See Annular Pancreas page for an explanation. |
||
|
28. The best imaging modality for acute pancreatitis is: A. US B. CT, no contrast C. Contrast enhanced CT (oral & IV) D. MRI C: See Pancreatitis page for an explanation. |
||
|
29. All the following are CT signs of pancreatitis except: A. Peripancreatic fluid collection & fat stranding B. Focal non-enhancing regions of the pancreas on contrast-enhanced CT C. Atrophic or enlarged pancreas with loss of normal internal structure D. Duct dilatation and strictures E. All of the above E: See Pancreatitis page for an explanation. |
||
|
||
|
||
|
32. The sentinel clot sign: A. Helps to localize the source of a hemopertioneum. B. Is due to the lower density of the clotted component of a hemoperitoneum. C. Is rarely seen. D. All of the above. A: The area of hemoperitoneum adjacent to a source of bleeding is most likely to clot first and may thus help localize the source of bleeding. The clotted component is MORE dense than the unclotted blood, not less dense. The sentinel clot sign is often seen. |
||
|
33. All of the following may be signs of free air in the abdomen EXCEPT: A. Double wall sign (Rigler's sign) B. Falciform ligament sign C. Football sign D. Ground glass sign D: The double wall sign describes the fact that both the inside and outside walls of bowel are visualized because they are outlined by air within the bowel and free air in the abdomen. The falciform ligament is visualized by free air in the abdomen. The football sign describes the shape of gas outlining the peritoneal cavity. The ground glass sign refers to the hazy appearance on plain film created by large amounts of fluid in the peritoneum. |
||
|
34. Imaging of hernias is best achieved by: A. Upper GI study then small bowel follow through. B. CT, ultrasound, or herniography, since either technique is equally effective. C. Depends on clinical scenario, with each imaging modality providing different strengths. D. CT, ultrasound, then MRI. C: The choice of imaging technique depends on the clinical scenario. Opacified herniated bowel loops may make diagnosis easy with CT scan, and CT is often useful to evaluate for an alternative disease process that may be mimicking a hernia. Real-time imaging with ultrasound and/or herniography may be preferable if specific maneuvers (i.e. Valsalva) elicit hernia symptoms. |
||
|
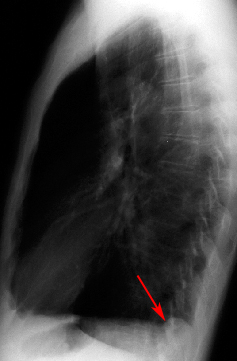
35. The following images demonstrates what type of hernia?
A. Morgagni hernia. B. Petit hernia. C. Grynfeltt hernia. D. Bochdalek hernia. D: Bochdalek hernias occur "back, and to the left" at the posterior aspectof the diaphragm, most often on the left. |
||
|
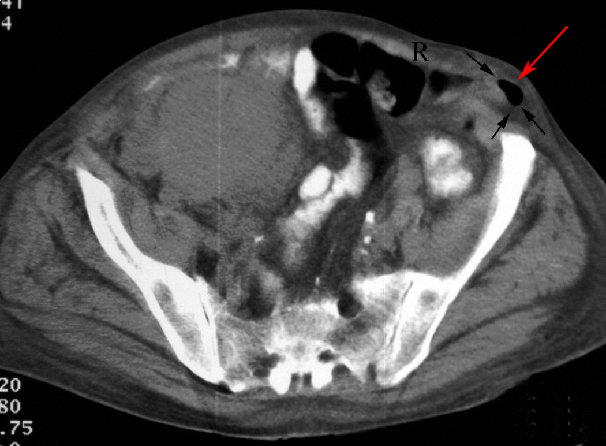
36. The following image demonstrates what type of hernia? (R=rectus abdominus)
A. Bochdalek hernia. B. Spigelian hernia. C. Femoral hernia. D. Direct inguinal hernia. B: Spigelian hernias occur through the anterior abdominal wall, lateral to the rectus abdominus. |




© Copyright Rector and Visitors of the University of Virginia 2013